

It is often said that love is blind but when faced with the harsh reality of sickle cell disease: should love persist in keeping its eyes shut, or courageously seek a path forward?
According to the Sickle Cell Foundation Nigeria, in Nigeria, the prevalence of sickle cell disorder is estimated to affect two out of every hundred children born, making us the largest number of people living with sickle cell disorder in the entire world.
This information suggests that a significant portion of the population, especially those with limited education, may still lack awareness of sickle cell disorder or show negligence towards it. Alternatively, it is possible that some educated individuals prioritize personal relationships over the potential risks associated with the disorder. Regardless of the reasons, it is the children who ultimately bear the consequences.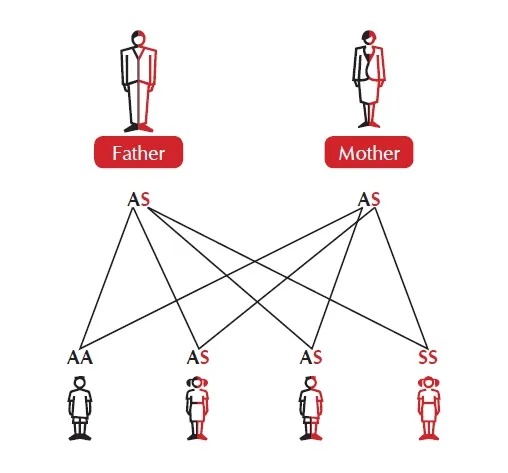
The sickle cell disorder is a genetic blood disorder that includes different types such as sickle cell anaemia (Hb SS), sickle hemoglobin C disorder (Hb SC), and sickle beta thalassemia (Hb SBthal). These conditions developed due to genetic mutations and became more common in regions with a high prevalence of falciparum malaria, which is the most dangerous type of malaria.
Because of its hereditary feature, the issue of genotypes and marriage is often taken seriously by doctors’ when counseling partners who intend to have children.
Genotype simply refers to the genetic makeup or combination of alleles an individual possesses. In humans, the genotypes for the hemoglobin gene constituents on red blood cells are AA, AS, AC, and SS. Among these genotypes, AC is uncommon, while AS and SS are considered abnormal.
While an ‘AA+AA’ couple and an ‘AA+AS’ couple is compatible, an ‘AS+AS’ couple or ‘SS+SS’ couple is widely frowned at. Yet, life happens and many couples are faced with the dilemma of helping their kids combat the disease.
The only solution left is a bone marrow transparent but it is terribly expensive, bears some risks and unavailable in Africa.
But even before considering the aforementioned option, couples who are both AS or SS still stand a chance to get married through two modern methods;
First, the Preimplantation Genetic Diagnosis (PGD) which is a laboratory procedure used in conjunction with in vitro fertilization (IVF) to reduce the risk of passing on inherited conditions. PGD uses IVF to mature and retrieve multiple eggs. These eggs, known as oocytes, are then inseminated with a single sperm using a technique called intracytoplasmic sperm injection.
The resulting embryos are allowed to develop in a controlled environment until they reach the six-to-eight-cell stage, which typically occurs on the third day of embryo development. At this stage, a small biopsy is performed, removing one to two cells from the embryo. It’s important to note that this biopsy process does not harm the remaining cells in the embryo. The extracted cells are then examined for specific genetic conditions. Embryos that are found to be unaffected by these conditions are transferred back to the woman’s uterus on the fifth day of embryo development, that is, only embryos without the sickle cell gene (SS genotype) are selected for transfer to the woman’s uterus.
The second method involves egg or sperm donation. This method comes in handy when two of the couples are carriers of sickle cell anaemia. They can opt for donated eggs or sperm from individuals who do not carry the sickle cell trait and by doing so ensure their kids are born without sickle cell disease.
Love in the end can still prevail over any odds including the sickle cell disorder. However, many are either not aware or incapable to afford its cost.

{kind=link}